





The ONE organ responsible for high blood pressure.
Persistent Pulmonary Hypertension of the Newborn (PPHN)
Persistent pulmonary hypertension of the newborn, or PPHN, occurs when a newborn's circulation system doesn't adapt to breathing outside the womb. While in the womb, the fetus receives oxygen through the umbilical cord, so the lungs need little blood supply.
After treatment for pulmonary hypertension, your baby's lungs will take weeks or even months to recover fully. It will be important to help protect your baby from catching colds or flu bugs.
Signs and symptoms
PPHN is often associated with the following signs and symptoms of perinatal distress:-
Asphyxia
-
Tachypnea, respiratory distress
-
Respiratory acidosis
-
Loud, single second heart sound (S2) or a harsh systolic murmur (secondary to tricuspid regurgitation)
-
Low Apgar scores
-
Meconium staining
-
Cyanosis; poor cardiac function and perfusion
-
Systemic hypotension
-
Symptoms of shock
Diagnosis
Suspect PPHN whenever the level of hypoxemia is out of proportion to the level of pulmonary disease. Clinically, PPHN is most often recognized in term or near-term neonates, but it can occur in premature neonates. Preductal and postductal oxygen saturation measurements via pulse oximetry will often show a 10% or higher gradient difference, which is dependent on the magnitude of left-to-right shunting at the foramen ovale (with preductual saturations being higher). It is important to note that these findings are not specific to PPHN and must be differentiated from structural heart disease. Echocardiography is considered the most reliable noninvasive test to establish the diagnosis, assess cardiac function, and exclude associated structural heart disease.Laboratory testing
-
Arterial blood gas levels (through an indwelling line [eg, umbilical arterial catheter or preductal peripheral arterial line]): To assess the pH, partial pressure of carbon dioxide (PaCO2) and the partial pressure of oxygen (PaO2) which might be higher in the preductal arterial line.
-
Complete blood cell count with differential: To evaluate for high hematocrit level (polycythemia and hyperviscosity syndrome may lead to or exacerbate PPHN); to determine whether an underlying sepsis or pneumonia is present
-
Coagulation studies (eg, platelet count, prothrombin time, partial thromboplastin time, international normalized ratio): To assess for coagulopathy (increased disease severity)
-
Serum electrolytes (eg, calcium) and glucose levels
Imaging studies
-
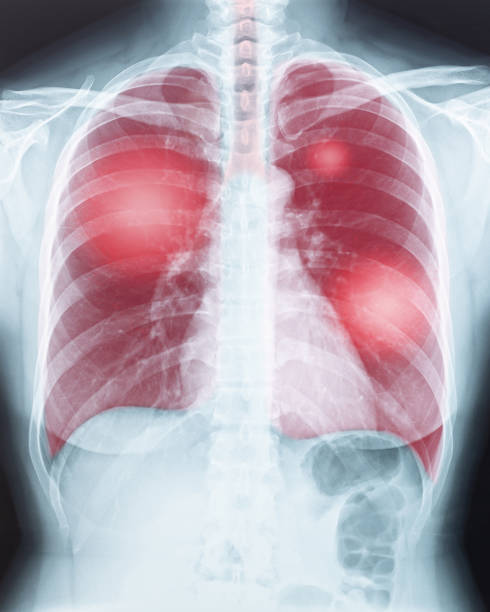
Chest radiography: To assess for presence of underlying parenchymal lung disease (eg, meconium aspiration syndrome, pneumonia, surfactant deficiency) and/or to exclude underlying disorders (eg, congenital diaphragmatic hernia); Persistent pulmonary hypertension of the newborn (PPHN). Meconium aspiration in a neonate. This radiograph was obtained shortly after birth and shows ill-defined, predominantly perihilar opacities in the lungs; these are more severe on the right than on the left. The lungs are hyperexpanded. The neonate's heart size is within normal limits.
-
Echocardiography: To screen and assist in making the diagnosis of PPHN and to rule out a structural heart lesion
-
Echocardiography with Doppler and color-flow mapping: To assess presence/direction of the intracardiac shunt at the ductus arteriosus and foramen ovale, as well as estimate the pulmonary arterial systolic/diastolic pressures
-
Cranial ultrasonography: To assess for intraventricular bleeding and for peripheral areas of hemorrhage or infarct if ECMO is being considered
-
Cranial ultrasonography with Doppler flow: To assess whether a nonhemorrhagic infarct is present
-
Brain computed tomography scanning or magnetic resonance imaging: To evaluate for central nervous system injury
Procedures
-
Cardiac catheterization: Rarely utilized to exclude congenital heart disease (eg, obstructed anomalous pulmonary venous return, pulmonary vein stenosis) because echocardiographic findings are typically diagnostic
Management
The treatment strategy for PPHN is aimed at maintaining adequate systemic blood pressure, decreasing pulmonary vascular resistance, ensuring oxygen release to tissues, and minimizing lesions induced by high levels of inspired oxygen and ventilator high pressure settings. General management principles include the following:-
Continuous monitoring of oxygenation, blood pressure, and perfusion
-
Maintaining a normal body temperature
-
Correction of electrolytes/glucose abnormalities and metabolic acidosis
-
Nutritional support
-
Minimal stimulation/handling of the newborn
-
Minimal use of invasive procedures (eg, suctioning)
Medical therapy
PPHN treatment may consist of the following:-
Inotropic support (eg, dopamine [first line in the absence of cardiac dysfunction], dobutamine, milrinone)
-
Surfactant administration: For premature and full-term newborns with parenchymal lung disease
-
Endotracheal intubation and mechanical ventilation: To maintain normal functional residual capacity by recruiting areas of atelectasis; to avoid overexpansion
-
High-frequency ventilation: Used in newborns with underlying parenchymal lung disease and low lung volumes; therapy is best in centers with clinicians experienced in achieving/maintaining optimal lung distention
-
Correction of hypoglycemia, hypocalcemia, acidosis, and alkalosis
-
Induced paralysis: Controversial; paralytic agents are typically reserved for newborns who cannot be treated with sedatives alone (Note: paralysis, especially with pancuronium, may promote atelectasis of dependent lung regions and promote ventilation-perfusion mismatch.)
Pharmacotherapy
-
Inhaled pulmonary vasodilators (eg, nitric oxide) and supplemental oxygen
-
Systemic vasodilators are potentially beneficial for chronic PPHN after the newborn period (eg, prostacyclin, phosphodiesterase inhibitors, endothelin receptor antagonists)
-
Prostaglandin E1 if the ductus arteriosus is closed or restrictive in the setting of suprasystemic pulmonary artery pressures and/or right ventricular dysfunction leading to poor systemic perfusion